Revenue integrity that starts before the chart closes.
Traditional revenue cycle starts after the chart closes—retrofitting codes to documentation that's already incomplete. Abridge starts in the room. One conversation captures the clinical detail that drives accurate risk adjustment, closes care gaps, and protects revenue.
Every code traced to the conversation
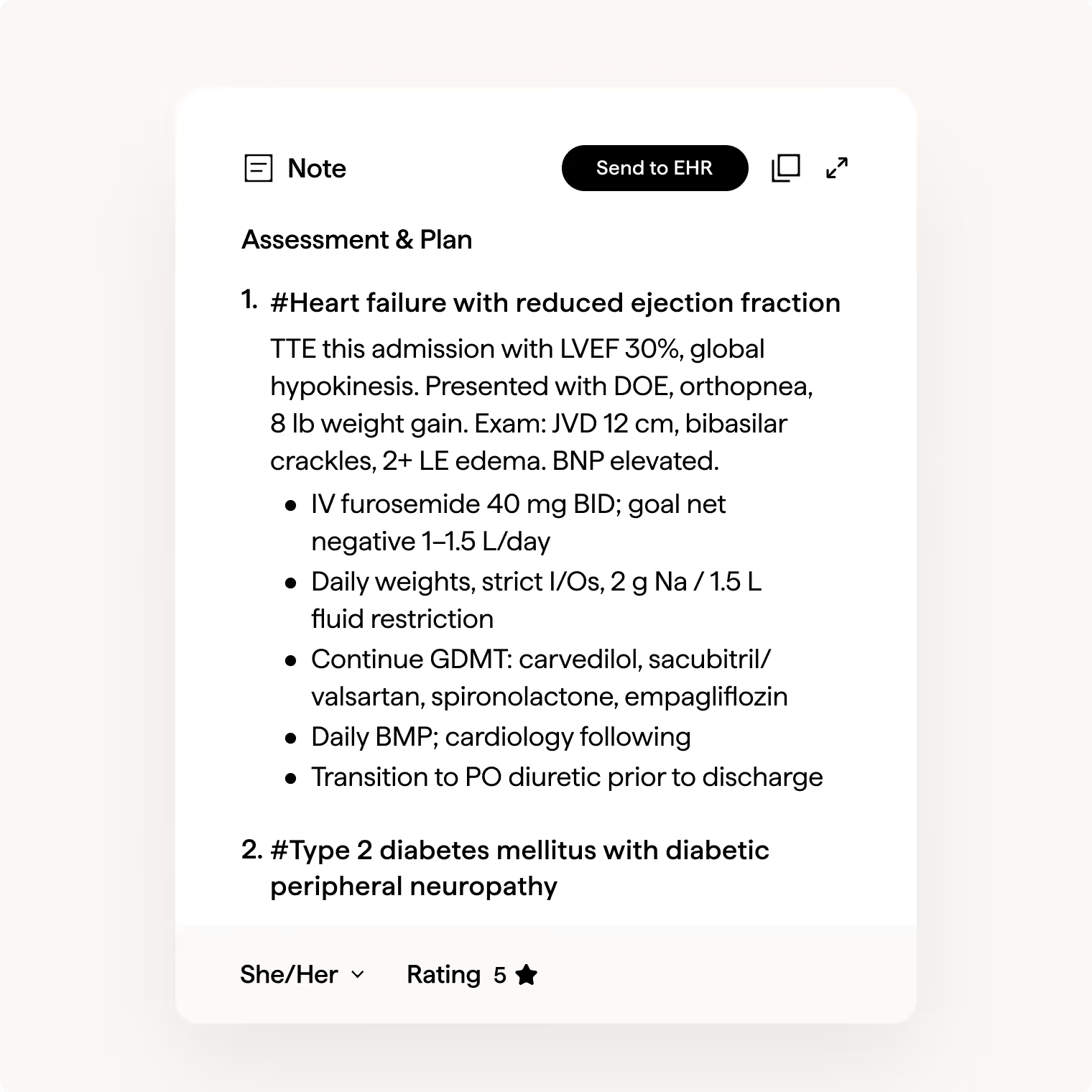
Documentation flows directly into existing clinical workflows. Every code and diagnosis is grounded in the clinical encounter so the record is complete, accurate and ready for billing before the clinician leaves the room.
Three product sets.
One platform.
No new workflows.
No new workflows.
Every Abridge RCM product deploys inside your existing EHR. Outputs land where they need to—diagnosis lists, billing workflows, downstream systems—without asking clinicians to change how they work.
Inpatient CDI delivered quietly—in the note, not after discharge
Traditional CDI review arrives days after the fact, while the physician has already moved on. Abridge surfaces specificity in-line as care happens, context carries forward across every note and every provider, and documentation is complete before anyone has to ask. No interruption. Fewer retrospective reviews.
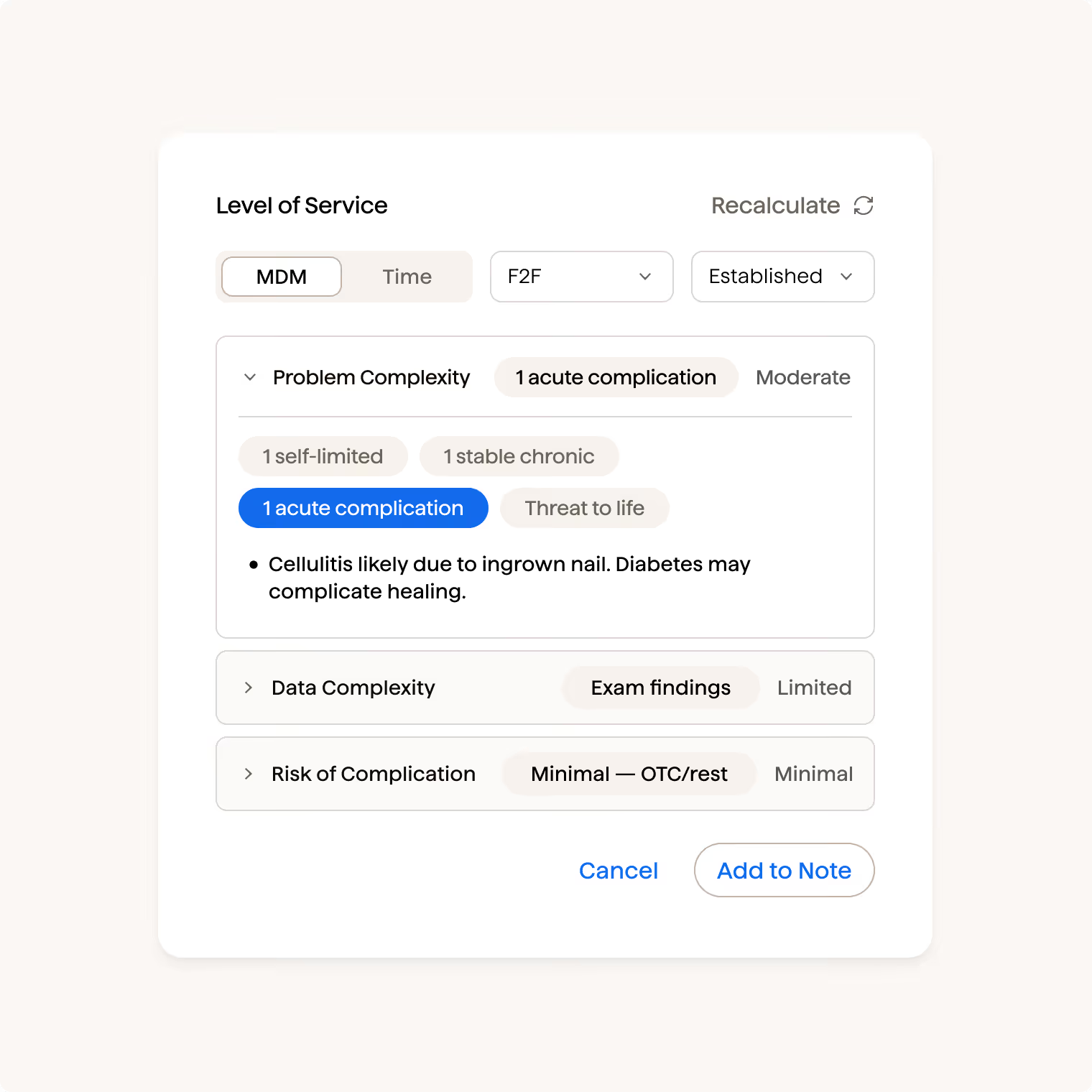
Ambulatory encounter integrity at the point of care
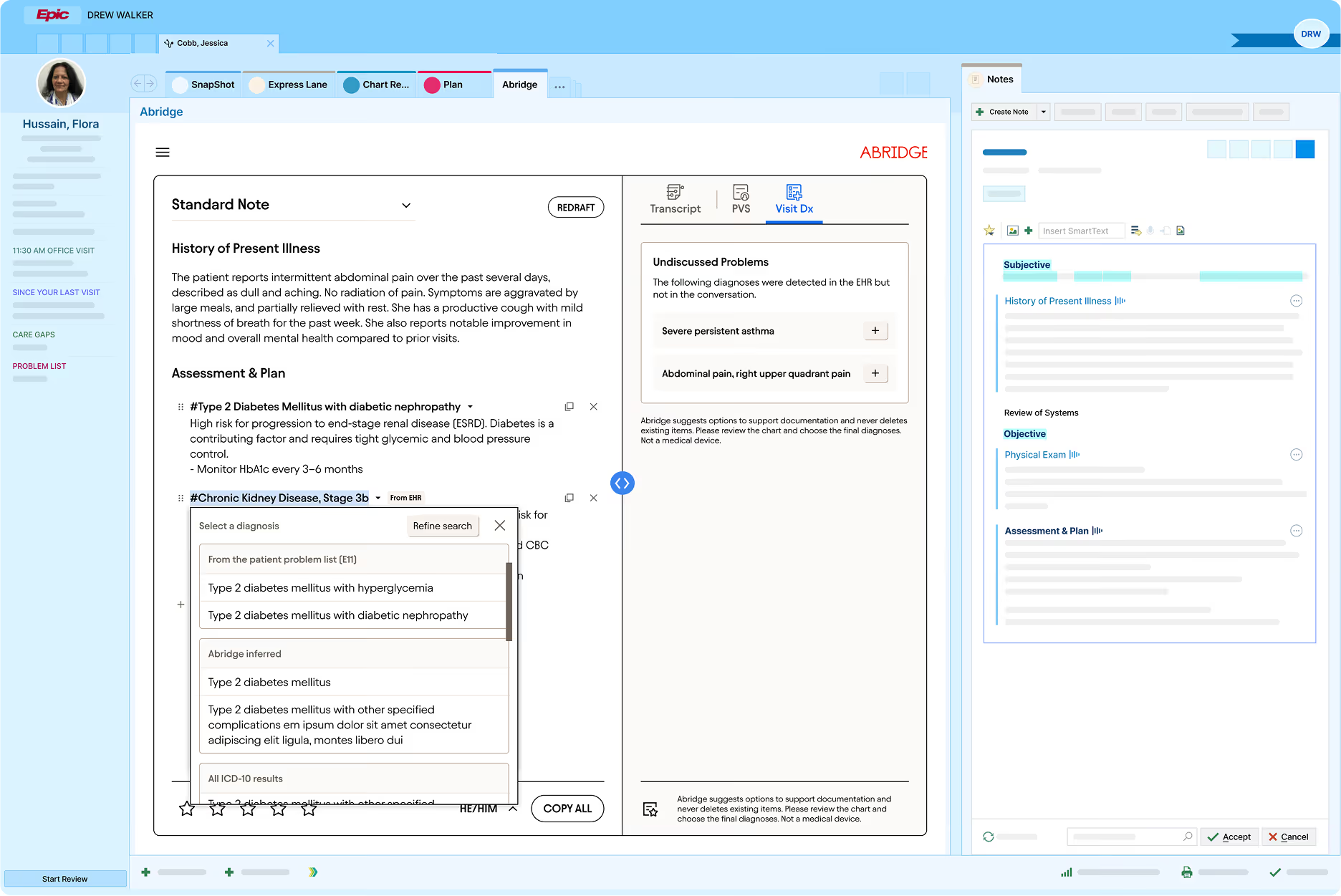
By the time a retrospective CDI query arrives, context has faded and the record already has errors. With Abridge ICD-10 and HCC codes surface in real time, E&M level calculates automatically, and visit diagnoses push back to the medical record before the note is signed. The loop closes before the clinician leaves the room.
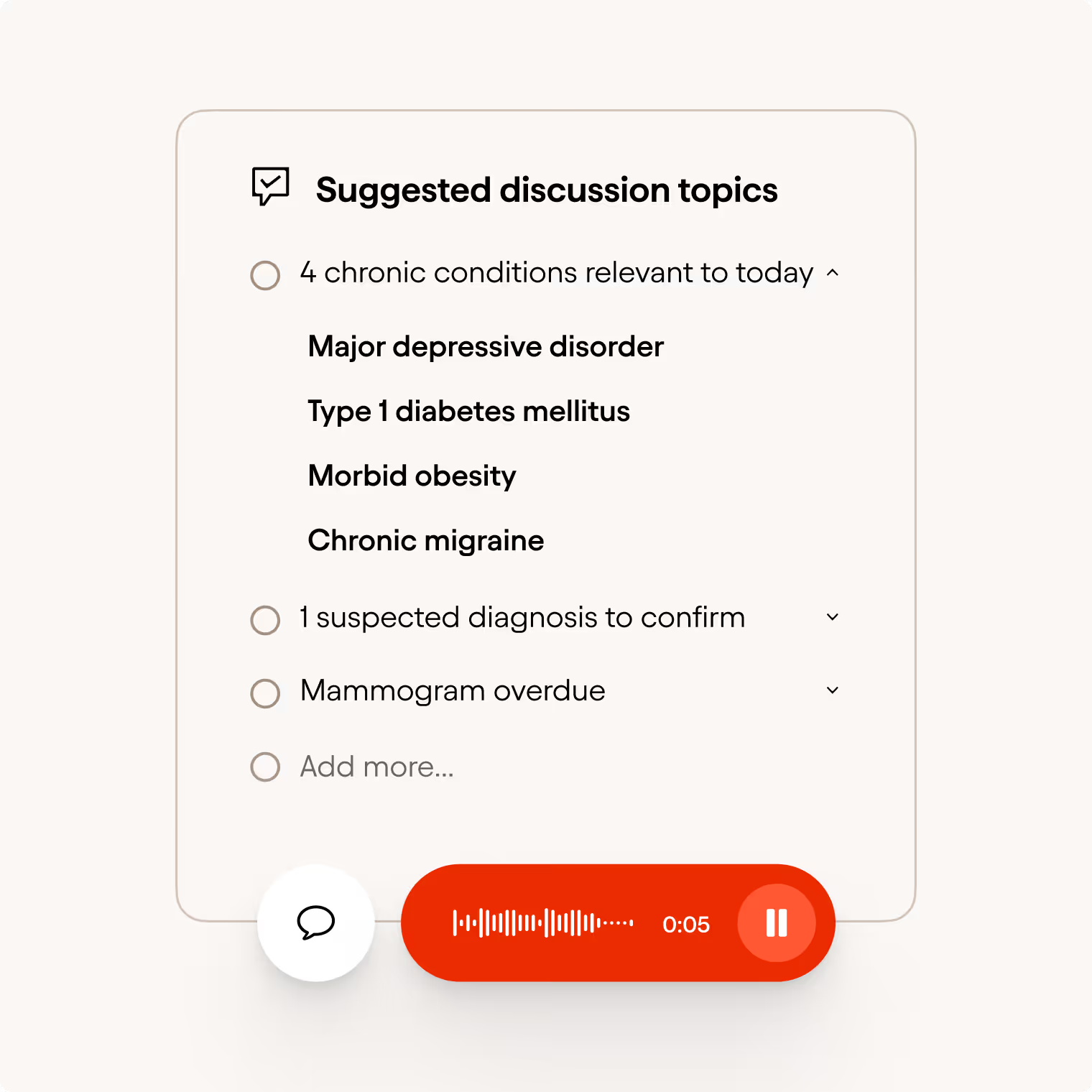
The right conditions addressed in the visit, not the back office
Most risk adjustment tools start from the chart, after care has been delivered. Abridge's Care Signals closes that gap at the source. Risk gaps map to each patient before the visit begins, conditions are tracked in real time as they're discussed, and documentation reflects the full scope of patient complexity before the note is signed. No separate portal. No manual flagging.
Intelligence at every point in the patient journey.
Most tools act once, retrospectively. Abridge works continuously—across every encounter, every stay, and every year of a patient's care.

Revenue intelligence built
from the conversation up
Most revenue cycle tools start after the fact. Abridge's RCM platform is architected differently, with every output starting from the clinical conversation.

Built from the note, not bolted onto it
Everything flows from the conversation. Not retrospective chart review. Not a separate workflow.

Before signature, not after discharge.
CDI intelligence surfaces in the conversation while documentation is still being written, not weeks later as a query.

Purpose-built for every care setting.
Outpatient, ED, and inpatient — with distinct capabilities built for each context, not one tool stretched thin.





.avif)