



How Geisinger Scaled Abridge to 1,000+ Clinicians in 10 Months
A Q&A with Dr. Ben Hohmuth, Chief Medical Informatics Officer and Clinical Lead for the Risant Value-Based Platform at Geisinger
When Geisinger adopted Abridge in late 2024, the organization didn’t start with a large-scale mandate or a complex rollout strategy. Instead, the approach was pragmatic: wait until the technology was ready, start with interested clinicians, and scale based on real demand.
After an initial pilot phase in late 2024, Geisinger expanded Abridge system-wide in early 2025, driving rapid adoption across the organization.
Dr. Ben Hohmuth, Chief Medical Informatics Officer and Clinical Lead for the Risant Value-Based Platform at Geisinger, focuses on improving clinician experience and optimizing workflows across the system. In this Q&A, he shares how Geisinger approached scaling Abridge, and where he sees ambient AI evolving across ambulatory, ED, and inpatient settings.
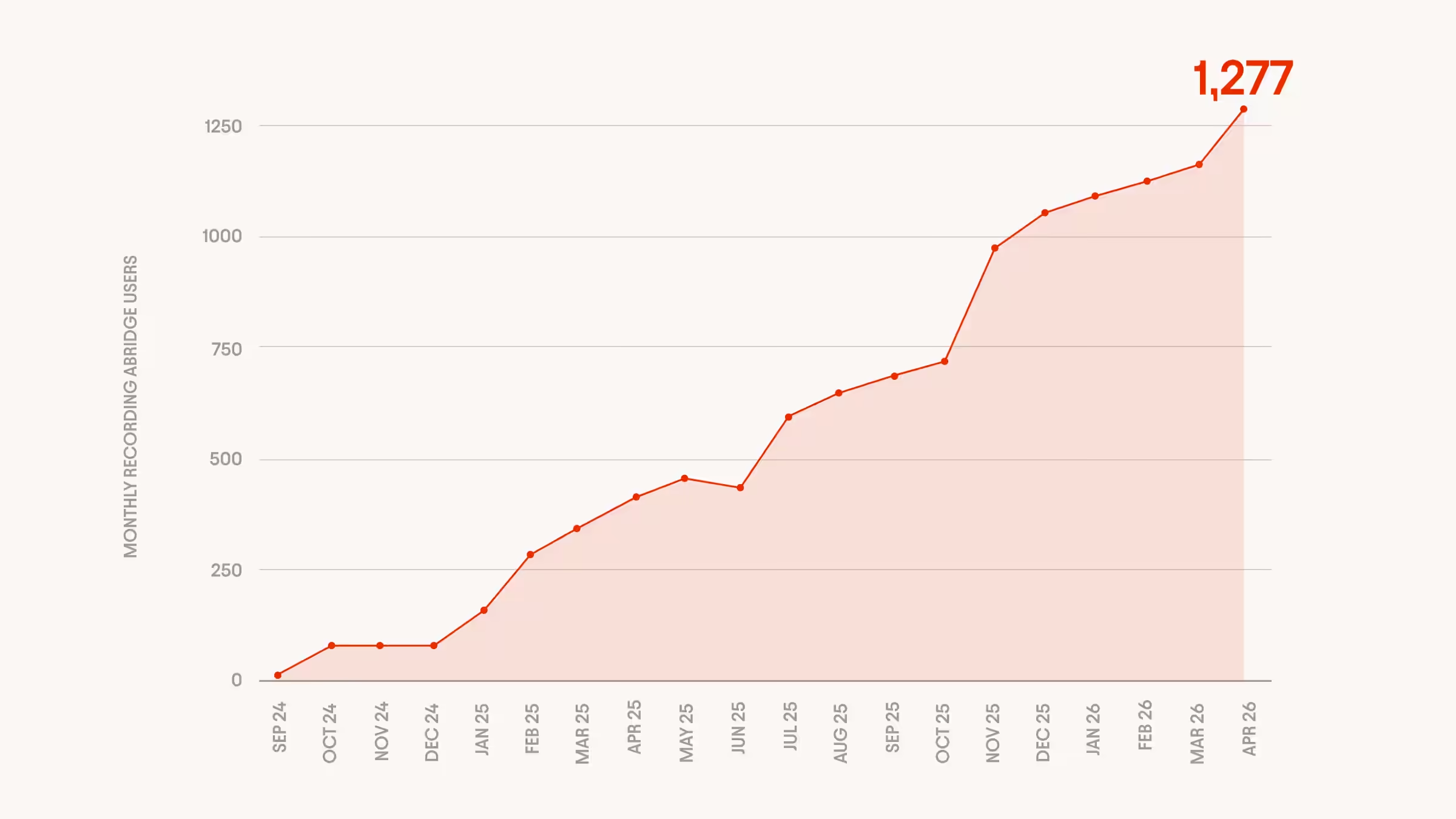
Seeing 187% growth in clinician adoption in just seven months (April–November 2025), Geisinger’s experience shows how quickly ambient AI can scale when clinicians see clear value and drive adoption themselves.
About Geisinger

In Conversation with Dr. Ben Hohmuth
How do you think about ambient AI more broadly within Geisinger?
Going early with AI is critical to the success of Geisinger in a lot of ways. We see it as a new way to solve problems that have been historically really challenging for us—around access, affordability, quality, and workforce.
Why did you decide to move forward when you did?
We had been tracking the space for a while, but it always felt like more of a niche thing—pilots here and there. It just didn’t feel like there was something we could scale until a couple of years ago. So a key thing we did was wait until there was something we felt really was enterprise-ready.
What did Geisinger’s rollout and expansion look like?
We went live with our first users in late September 2024, and surpassed 1,000 users by November 2025. Now, every physician, APP, resident, and fellow at Geisinger has access to Abridge if they want it.
How did you approach initial adoption?
We started with a small group of clinicians who were really interested. The initial plan was to identify people who needed it—people who take a long time to complete notes, write long notes, or don’t close charts on time.
What helped drive that demand?
If you have something that really has an impact, once people start using it, word spreads and people want it. You don’t have to sell it or convince them.
A lot of the trust was created by peer communities. We set up a Teams channel that everyone was on, and people started teaching themselves. They would ask questions, and instead of us answering, their colleagues would answer. That happened pretty quickly.
What did implementation look like in practice?
We kept it simple. We’re an Epic shop with one instance across the organization, so you open Epic on your phone and go. We had training available in our learning management system, but we didn’t make it required.
Overall, we tried to decrease the barriers as much as possible: short how-to guides, basic setup, and letting people get started quickly.
What did you learn about how clinicians actually use Abridge?
One thing we learned early is that usage isn’t always what you expect. For example, some pediatricians were using it maybe 20% of the time, but they were still seeing improvements. When we looked into it, most of their visits are templated well-child visits—they don’t need ambient AI for that.
They were using Abridge for the 25% of visits that are more complex and take more time and cognitive effort. And that’s where it had an impact. So we’re still figuring out what the right thresholds are, because there are specialties where lower usage still delivers a lot of value.
How did you think about ROI and success metrics?
We look at both objective and subjective measures—things like time spent in notes, and also survey data on burnout and work outside of work.
We saw an average decrease in time in notes of about 45 minutes per 8 hours of scheduled patients. For primary care, self-reported burnout and work outside of work both went down by about 50%.
However, from the beginning, we were not primarily fixated on demonstrating financial ROI in hard dollars. This is about improving clinician experience first and foremost, so we’re more interested in tracking metrics like burnout, pajama time, and things like that. Productivity expectations may change but this would be an enabler rather than a quid pro quo.
Have clinicians changed how they use it over time?
Yes, people are getting more savvy. Part of this is prompt engineering, even if they don’t call it that. For example, some clinicians will start the recording a little early and give context about what they’re about to do. That improves the output. So the software is getting better, and the clinician users are getting better too!
How did you approach governance and scaling?
We started with centralized management of licenses. We wanted to be good stewards, but also clear that this wasn’t about tying usage to productivity expectations.
We didn’t want a situation where, if people became more efficient, someone else would say they should just see more patients. That wasn’t the goal.
The tools we have to govern and monitor are lagging behind the technology we have in use. We’re figuring out the best way to manage licenses efficiently as demand grows.
What matters most in the way you evaluate new AI tools?
We need to be problem focused. What use case are we talking about? That discipline matters. A lot of times people want to talk about AI first, but the real question is what problem we’re actually trying to solve.
We also try to stay enterprise-first. If a capability already exists in one of our core platforms and it meets most of the needs, that may be the right answer. We’ve invested in those tools, and if it meets 80% of the need, that’s good enough.
How are you thinking about AI governance more broadly?
This is a work in progress area of rapid iteration for us, trying to strike the right balance in our AI portfolio between responsible use and rapid expansion. We want both. With regards to ambient documentation, questions about accuracy or hallucinations come up, but those issues existed before, whether it was human dictation, voice-to-text, or templates. The key is that there’s a human in the loop, and when they sign the note, they’re responsible for it. That’s still true here.
What role does partnership play in this kind of rollout?
Responsiveness matters. It matters that there’s a feedback loop and that issues can be raised and addressed quickly. With tools like this, the ability to iterate is important, because the technology and the workflows both continue to evolve.
What’s your view on where this is going?
Synthesizing what comes from the conversation with what comes from the chart, and from other knowledge resources, is something I’m really excited about. I think there are three really important data sets: the conversation with the patient, the information in the chart, and clinical knowledge. We’ve had tools that work on each of those separately.
What’s the biggest takeaway from your experience?
Start with the willing. If the technology has real impact, adoption will follow. And a lot of that adoption will come from clinicians talking to each other, not from top-down direction.