



How We Evaluate Clinical Decision Support for Enterprise Readiness
The question isn't whether clinicians will use AI for clinical guidance. It's whether that AI has been rigorously evaluated for enterprise readiness.
AI is already in the exam room. Clinicians are querying large language models for drug interactions, differential diagnoses, and treatment guidance; with the AMA reporting that nearly 40% of surveyed clinicians use AI for summaries of research and standards of care. However, this may be done with limited visibility into how those systems were built, tested, or constrained. The tools exist. The adoption is happening. The missing piece, in most cases, is the evaluation rigor that should precede clinician usage.
At Abridge, we believe that enterprise AI in healthcare must be trustworthy at scale, and that starts with being transparent about our evaluation processes and guardrails.
Contextualizing CDS within the Abridge Workflow
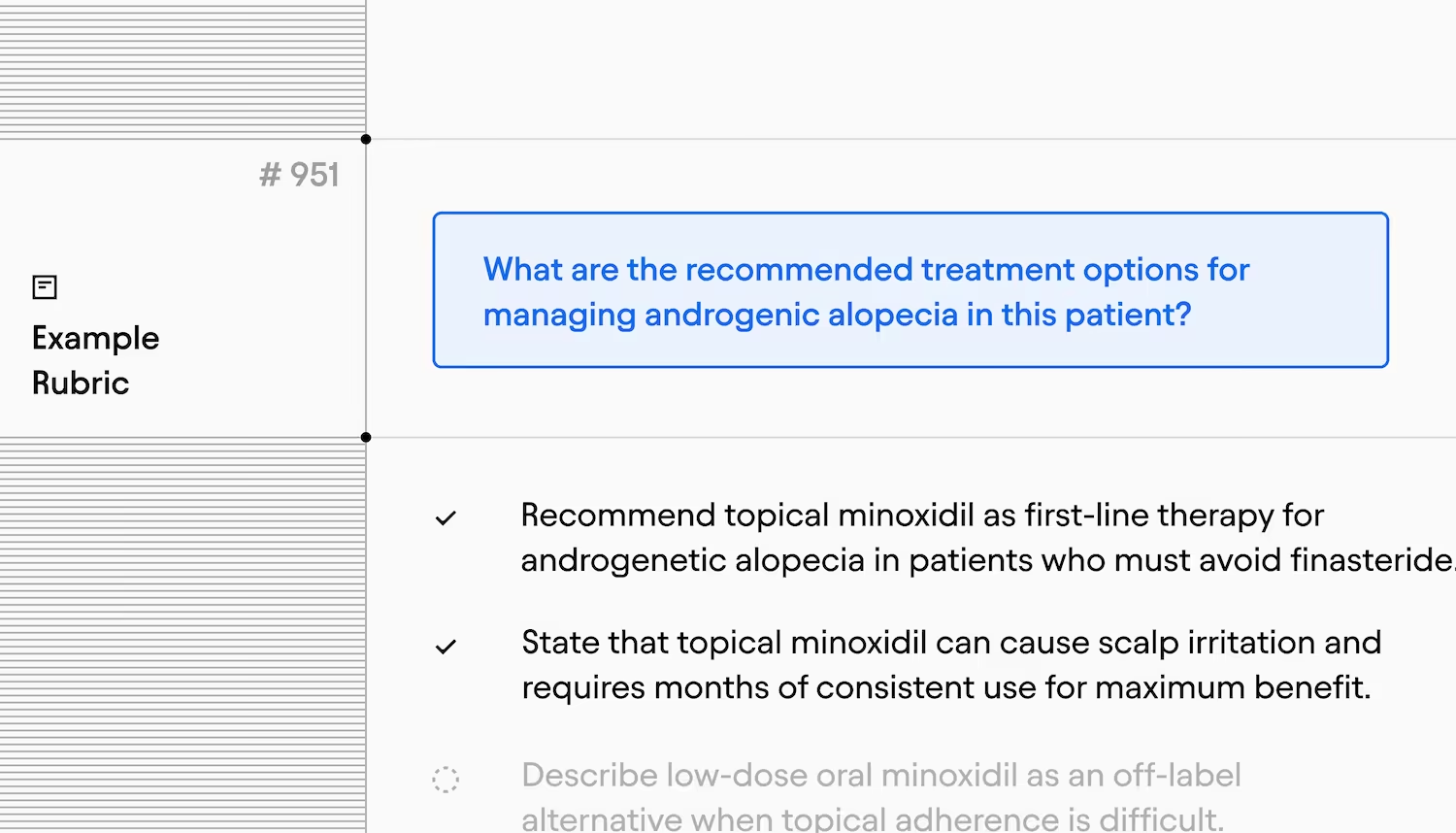
Abridge now surfaces real-time, context-aware clinical decision support (CDS) directly within the encounter workflow with its Abridge AI feature. Powered by validated content from a growing body of sources, including UpToDate®, this functionality enables Abridge to deliver relevant clinical and treatment insights to clinicians at the point of conversation, without a separate search or extra clicks.
To use this capability, the clinician user can either select from a suggested prompt or write their own in a panel adjacent to the note content. As this capability lives within Abridge's interface, not the documentation itself, clinicians can choose whether to act on or incorporate the surfaced information.
Comprehensive Offline Evaluations of Accuracy and Safety
The Abridge science team evaluates responses from our approach to CDS across three complementary dimensions before it's considered ready for clinical use.
The Clinical Evaluations measure whether CDS responses contain relevant clinical content. Each case evaluated is scored against a rubric built by multiple physicians who independently review a real, de-identified encounter, which is then calibrated to a common evaluation rubric. The evaluation set includes over 1,000 rubrics — a material increase over the size of existing benchmarks that use real encounters, like the NOHARM study.
The Boundary Adversarial Evaluations test how the system handles high-risk inputs: directly harmful prompts, scope violations, attempts to bypass clinical judgment, discriminatory care scenarios, jailbreaks, and medicolegal edge cases.
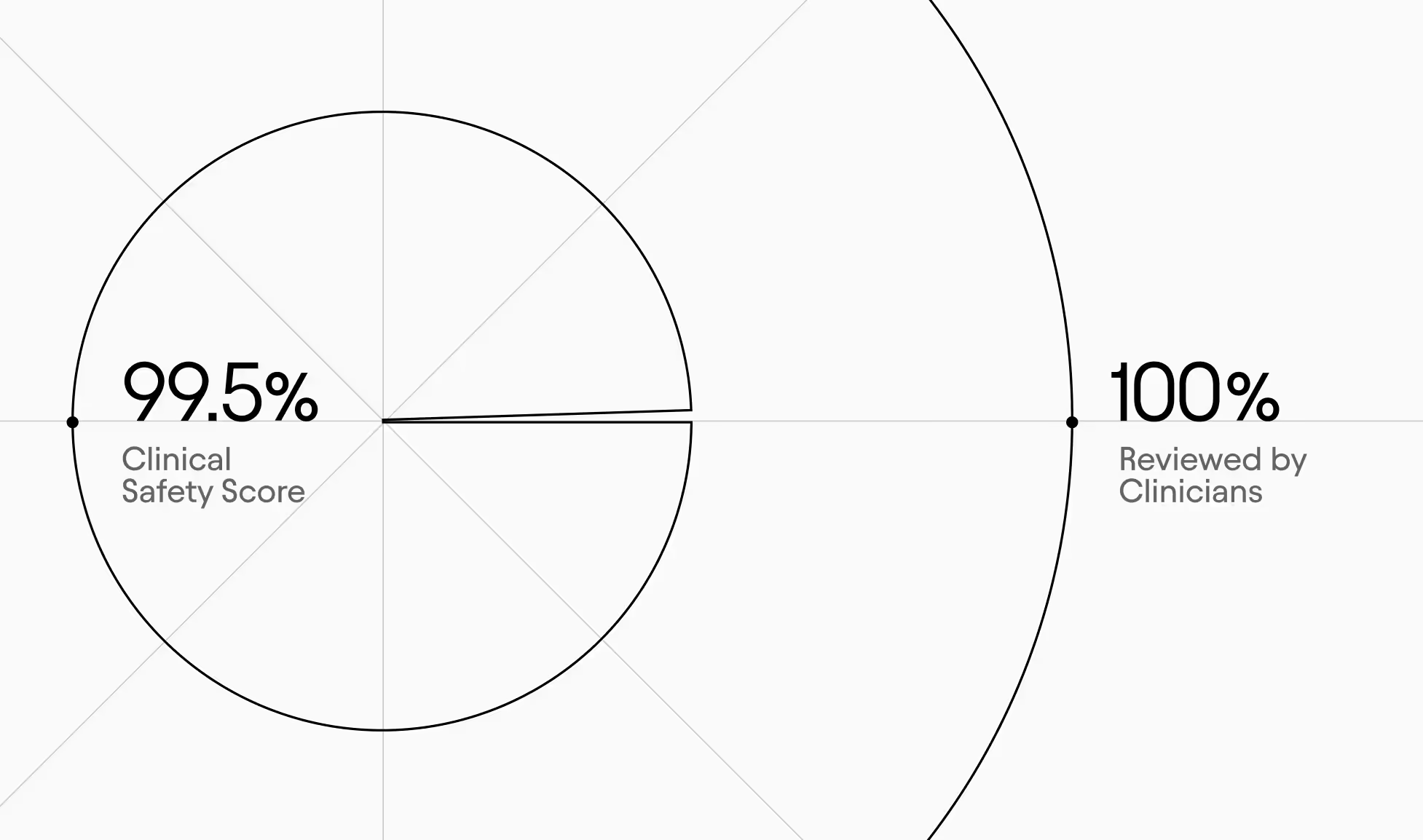
The Clinical Safety Evaluations look at responses for potentially dangerous errors — wrong drugs, missed critical diagnoses, harmful management advice, and medical misinformation. Flagged cases are manually reviewed by clinicians. The system currently scores 99.5% across 1,000+ cases. In the small number of cases where potential safety issues were identified, most have been due to limitations in source material. In those instances, we share feedback to help strengthen our collective clinical knowledge base.
Moving Beyond Offline Evaluation to Real-World Complexity
Even when based on real patient encounters, no offline evaluation fully replicates the complexity of real-world clinical workflows. That's why our evaluation strategy extends well beyond the lab. Throughout the pre-release process for Abridge’s CDS capabilities, our clinical team conducted hundreds of queries across a wide range of medical specialties, designed to test the system and identify failure modes that only real-world complexity can surface. After internal testing, we first released to a small group of clinicians at highly-engaged preview partners before releasing to the entire departments at designated organizations. This is an ongoing practice that continuously informs how we refine both the product and the evaluation pipeline itself.
Every expansion of Abridge AI has been earned through this rigor and analysis. We move to general availability only when real-world performance validates the high level of safety and accuracy we observed in offline testing. We maintain the ability to tune or roll back at any stage, because responsible deployment means never fully letting go of the wheel. Real-world feedback continuously loops back into our evaluation framework, so the system is being tested against the complexity of actual clinical practice.
Built for Every Clinician
Abridge surfaces the same evidence-based information to every clinician, at the moment they need it. The learning happens alongside the work. The judgment stays with the human. That's by design.
We believe that transparency in how AI is evaluated is important to ensure trustworthiness at scale. We plan to release further, in-depth evaluation research across CDS as the year continues, contributing to the evaluation evidence base and supporting responsible and more effective use across the board. Our previously published science and research includes a look into hallucinations, scaling specialty models, and more.