



Why HonorHealth Skipped the Pilot and Went Straight to Enterprise-Wide AI with Abridge
With Dr. Matthew Anderson, CMIO, HonorHealth
After a three-and-a-half-year search for the right ambient AI solution, HonorHealth selected Abridge to support 500 clinicians across ambulatory and inpatient settings without running a traditional pilot.
Overview
Based in Arizona, HonorHealth is a rapidly growing health system serving a population of over 5M annually with 9 acute-care hospitals and over 200 care locations across greater Phoenix and Florence. As documentation burden and after-hours “pajama time” increased, leadership began looking for a solution that could reduce friction for clinicians across all care settings.
Previous attempts with other vendors fell short—either clinicians rejected the tools outright or the economics didn’t work. With Abridge, HonorHealth found a partner that met the bar across integration, usability, scalability, and cost, along with strong validation from peer health systems.
Rather than piloting the technology, HonorHealth took a different approach: a full enterprise rollout beginning January 2026, with a wave-based strategy designed to drive adoption quickly.
In this conversation, Dr. Matthew Anderson, Chief Medical Information Officer, shares why HonorHealth skipped the pilot phase, how they structured the rollout for success, and what impact they’re seeing so far.
In Conversation with Dr. Matthew Anderson

How did HonorHealth approach finding the right ambient AI solution?
This has been a multi-year journey for us. We started because our clinicians were struggling. You could see it in the data. You could see how much time they were spending in notes, how much time they were spending at home, that “pajama time.” We needed something better.
We tried another ambient vendor, and it failed. Our clinicians told us very clearly: “I don’t want this. Take it off my phone, take it off my computer.” And physicians aren’t shy—we’ll tell you what works and what doesn’t.
Then we looked at another partner, and we just couldn’t make the finances work. At the same time, we realized this couldn’t just be for physicians in ambulatory care. If we were going to do this, we needed to support inpatient clinicians and nurses, too.
There were very few partners that checked all the boxes: strong EHR integration, a stellar track record with physicians, the ability to expand to nursing, and a price point that made sense. That’s where Abridge really stood out.
Why did you decide to skip a pilot and go straight to enterprise rollout?
Truthfully, you have to burn the boats. If we were going to do this, we had to commit. We signed an enterprise-wide contract and said, we’re going to make this work. No retreat.
“We were interviewing physicians and they were asking, ‘What’s your ambient solution?’ And we didn’t have one. It’s like asking someone to do their job without the internet.”
The other thing is pilots don’t actually reduce the work. Whether you’re putting five people on or 500 people on, it’s the same effort for the IT team. So if you’re going to do the work, you might as well run. Pilots can sometimes be a soft yes. We wanted a hard yes.
How did you structure the rollout to drive adoption?
We tend to do things a little differently. The normal way is you go building by building, specialty by specialty. But the normal thing gets you normal results, and we wanted something better.
So we took a wave-based approach and were very intentional about the first group. We focused on leadership—clinical leaders, informatics, innovation—because if I’m not going to use it, I’m not going to ask anyone else to use it.
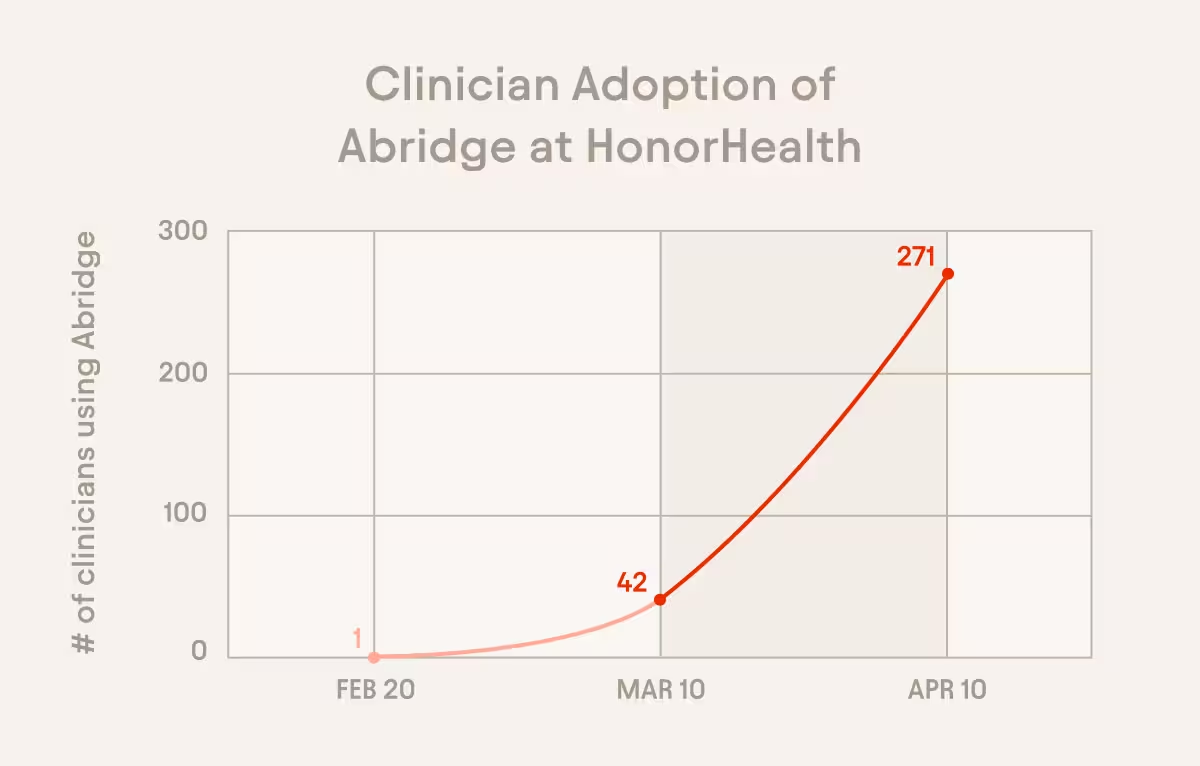
We also made it multi-specialty. Every specialty is struggling. No one group has a monopoly on burnout, so it didn’t make sense to prioritize one over another. What happens is you create your own ambassadors. You get your early adopters in, and they pull everyone else along. By the time we launched our second wave, we had close to 300 clinicians, and now we already have a waitlist for wave three.
What has clinician feedback looked like so far?
It’s been immediate. We set up a Teams channel for troubleshooting, but by the end of day one, it turned into people saying, “I love this, don’t ever take it away.” We were seeing messages like, “This is a game changer.”
One story I shared with our executives was about an oncology leader. He told me upfront, “This isn’t going to work for oncology. Just give my license to someone else.” He tried it anyway. After about a month, he came back and said it had changed his practice. He’s spending more time with patients, and, for the first time in his career, he’s closing his notes the same day. Now he’s telling everyone else to use it.
Did anything about adoption or perception surprise you?
I think clinicians are right to be skeptical. We’ve been told for years that technology is going to make things better, and a lot of times it hasn’t. EMRs are a good example—you get more clicks, not less.
There’s also this idea that every specialty is different, so how could one solution work for all of them? But it’s a little like that Henry Ford quote. If you ask people what they want, they’ll say faster horses. You don’t realize what a car is until you’re actually in it. And once you’re in it, it changes everything.
Have you seen an impact on recruitment or patient experience?
Yes, on both. From a recruitment standpoint, this is becoming table stakes. We have clinicians coming from other health systems asking, “Why don’t you have this?” That creates pressure pretty quickly.
On the patient side, I think this is the part people underestimate. If clinicians are more present and not focused on the computer, that changes the experience. And in healthcare, word of mouth matters. It costs more to acquire a patient than to keep one. If you make that experience better, patients stay.
How are you thinking about ROI and measuring success?
There are a few things we’re looking at. First, we want clinicians to maintain their productivity, but with less effort in the EMR. Same output, less friction.
From a financial standpoint, faster chart closure matters. The faster you close a note, the faster you get paid. That’s just a basic fact in healthcare.
We may also see some increase in patient volume, not because we’re asking for it, but because clinicians have more capacity.
And then there’s patient experience and retention, which are harder to quantify but just as important.
We’re also doing pre- and post-surveys with KLAS to get a broader view of the impact.
At the end of the day, you’re looking for a win across the board—for clinicians, patients, and the organization. I may not need every data point to believe in it, but my CFO probably will.
This interview was edited for length and clarity.